The most common form of inherited ataxia is commonly misdiagnosed1,2
Friedreich ataxia (FA) can present with nonspecific (such as balance and coordination disturbances) or atypical symptoms, making it common for the condition to be overlooked and misdiagnosed.2,3
Determining the etiology of ataxia
Ataxias can be broadly categorized as acquired, genetic, or idiopathic.4
Because ataxias—even inherited ataxias—can present at almost any age with or without family history,5 it is important to perform a thorough evaluation to determine the etiology. Click through this high-level process flow to see considerations for diagnosing the root cause of ataxia.
Acquired4,6
Autoimmune
Cancer
Infection
Metabolic
Nutritional
Toxic
Genetic4
(familial, hereditary)
Dominant
Recessive
X-linked
Mitochondrial
Idiopathic7
(sporadic)
Determining the cause of ataxia
Acquired, genetic, or idiopathicEtiology insights7,8:
- Acquired ataxias may be immune-mediated, degenerative, caused by deficiencies, or associated with infections. They could also be the result of prolonged exposure to environmental toxins
- Genetic ataxias like FA are inherited from the patient’s parents. There are several potential inheritance patterns, characteristic of specific genetic ataxias, that could help narrow down the cause of the ataxia
- Idiopathic ataxias are ataxias with no known cause
Signs that may be present in patients with ataxia2,7,8:
- Gait ataxia—impairment of the ability to coordinate the movements required for normal walking
- Dysarthria—speech disorder that occurs when the muscles used for speaking are weak or difficult to control
- Square Wave Jerks—a condition similar to but different from nystagmus, when saccadic intrusions separated by pauses cause involuntary, rapid, and repetitive eye movements
- Intention tremor—involuntary, rhythmic shaking that occurs when making a purposeful movement, like reaching for something
- Dysmetria—difficulty in performing controlled, accurate movements
- Dysdiadochokinesia—difficulty in performing rapid, alternating movements like finger taps
Patient considerations
Age of onset, rate of progression, family historyEtiology insights:
- Rate of progression could suggest a possible etiology for a patient’s ataxia8
- Faster progression with noticeable changes within a few months could suggest a possible structural cause, such as a tumor, or an immune-mediated ataxia such as paraneoplastic spinocerebellar degeneration
- Family history can help determine a possible genetic cause and inheritance pattern8-10
- Patients with a long family history of ataxia may have a condition with an autosomal dominant inheritance pattern
- Patients with no family history, or who have a sibling with similar symptoms, may have a condition with an autosomal recessive inheritance pattern
FA considerations:
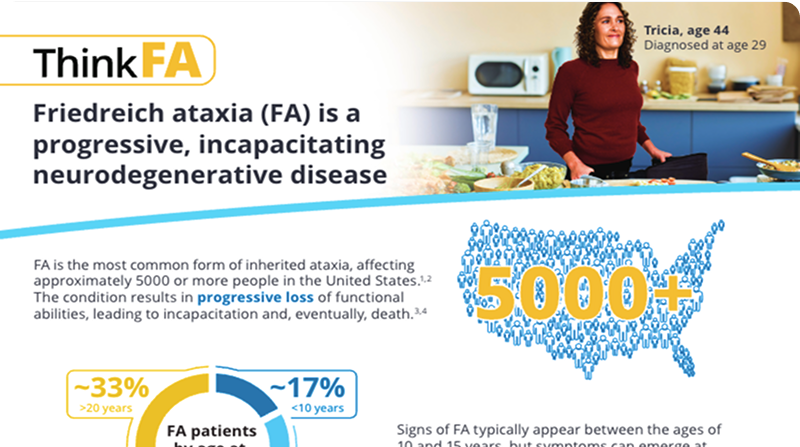
- Though FA symptoms often emerge during childhood and adolescence, onset can occur at nearly any age2
- As many as 1 in 3 FA patients receive their diagnosis as an adult1
- Age of onset can affect the symptoms with which a patient with FA presents2,11,12
- A younger age of onset typically includes classic FA symptoms, such as gait ataxia, loss of reflexes, loss of vibrational sense in the lower limbs, and poor proprioception. Issues like scoliosis or cardiomyopathy may be more apparent in these patients
- An older age of onset may include less common FA symptoms such as chorea or spasticity. Cardiomyopathy and scoliosis may be mild or not present
Diagnostic evaluations
Blood and urine studies, diagnostic imagingEtiology insights:
- Blood and urine studies can be useful in ruling out possible causes such as gluten ataxia (”Celiac Brain”) or vitamin imbalance (vitamin E)8,13
- Diagnostic imaging, including magnetic resonance imaging (MRI) and computed tomography (CT) scan, may be able to determine whether the ataxia has been acquired through a structural cause8
- Tumor, stroke, or lesions in the brain may cause symptoms of ataxia
FA considerations:
- Buccal cell samples and whole blood panels can identify levels of the frataxin protein in the body, which may suggest FA14
- FA may be suggested in the results of an MRI8
- Thinning of the cervical spinal cord and cerebellar atrophy are characteristic of FA
- Cerebellar atrophy may be more apparent in later-stage patients
Confirmatory genetic testing
GAA triplet-repeat expansion analysis, FXN sequencingEtiology insights8:
- Among genetic ataxias, there are 4 primary modes of inheritance
- Autosomal dominant (1 parent can pass on a mutated gene)
- Autosomal recessive (2 parents must pass on a mutated gene)
- X-linked (the mutation appears on the X chromosome)
- Maternal mitochondrial inheritance (mutations in the mitochondria inherited from the mother)
FA considerations:
- FA is passed on through an autosomal recessive inheritance pattern15
- GAA expansion testing is the first step in genetically confirming a diagnosis of FA16
- Whole-exome or next-generation sequencing does not identify GAA expansions and may return a normal result in patients with FA
- About 4% of patients may require FXN sequencing to additionally identify a mutation in the other allele of the FXN gene16
Explore FA further
This downloadable resource may be helpful for identifying and diagnosing potential patients with FA.
FA Signs and Symptoms One-Page Summary
High-level summary on FA, most common symptoms, and how to confirm a diagnosis with genetic testing
Differential diagnoses of FA
There are several other conditions with symptoms that are similar to FA, but a close look at certain areas can help identify the differences and find a correct diagnosis.
| Feature | Friedreich ataxia10,17 | Multiple sclerosis18‑21 | Charcot-Marie-Tooth disease22‑25 | Cerebral palsy26‑31 |
|---|---|---|---|---|
| Age of onset | ~10 to 15 years (range: ~2 to >50 years) | 20 to 40 years | ~5 to 25 years | <1 year |
| Brain atrophy | Advanced cases only (cerebellar) | Frequent | Rare or absent | Atypical (<10% cerebellar) |
| Pyramidal signs | Frequent | Present | Present | Frequent |
| Peripheral neuropathy | Present (sensory axonal) | May be present | Frequent | Atypical |
| Cardiomyopathy | Present | Absent | Absent | Absent |
| Associated gene(s) | Frataxin (FXN) | Unconfirmed | Polygenic | Polygenic (14% of cases) |
| Friedreich ataxia10,17 | Multiple sclerosis18‑21 |
|---|---|
| Age of onset ~10 to 15 years (range: ~2 to >50 years) |
Age of onset 20 to 40 years |
| Brain atrophy Advanced cases only (cerebellar) |
Brain atrophy Frequent |
| Pyramidal signs Frequent |
Pyramidal signs Present |
| Peripheral neuropathy Present (sensory axonal) |
Peripheral neuropathy May be present |
| Cardiomyopathy Present |
Cardiomyopathy Absent |
| Associated gene(s) Frataxin (FXN) |
Associated gene(s) Unconfirmed |
| Friedreich ataxia10,17 | Charcot-Marie-Tooth disease22‑25 |
|---|---|
| Age of onset ~10 to 15 years (range: ~2 to >50 years) |
Age of onset ~5 to 25 years |
| Brain atrophy Advanced cases only (cerebellar) |
Brain atrophy Rare or absent |
| Pyramidal signs Frequent |
Pyramidal signs Present |
| Peripheral neuropathy Present (sensory axonal) |
Peripheral neuropathy Frequent |
| Cardiomyopathy Present |
Cardiomyopathy Absent |
| Associated gene(s) Frataxin (FXN) |
Associated gene(s) Polygenic |
| Friedreich ataxia10,17 | Cerebral palsy26‑31 |
|---|---|
| Age of onset ~10 to 15 years (range: ~2 to >50 years) |
Age of onset <1 year |
| Brain atrophy Advanced cases only (cerebellar) |
Brain atrophy Atypical (<10% cerebellar) |
| Pyramidal signs Frequent |
Pyramidal signs Frequent |
| Peripheral neuropathy Present (sensory axonal) |
Peripheral neuropathy Atypical |
| Cardiomyopathy Present |
Cardiomyopathy Absent |
| Associated gene(s) Frataxin (FXN) |
Associated gene(s) Polygenic (14% of cases) |
Download Epic and Cerner EHR Resources
Genetic testing is the most effective way to confirm a diagnosis when you suspect FA32
References
1. Donoghue S, Martin A, Larkindale J, Farmer J. A meta-analysis study to evaluate time to diagnosis of Friedreich’s ataxia in the U.S. Friedreich’s Ataxia Research Alliance; 2018. 2. Parkinson MH, Boesch S, Nachbauer W, Mariotti C, Giunti P. Clinical features of Friedreich’s ataxia: classical and atypical phenotypes. J Neurochem. 2013;126(suppl 1):103-117. 3. Indelicato E, Nachbauer W, Eigentler A, et al. Onset features and time to diagnosis in Friedreich’s ataxia. Orphanet J Rare Dis. 2020;15:198. 4. Sarva H, Henchcliffe C. Ataxia & cerebellar disease. In: Brust JM, ed. CURRENT Diagnosis & Treatment: Neurology. 3rd ed. McGraw-Hill Education; 2021. Accessed December 14, 2024. https://accessmedicine.mhmedical.com/content.aspx/bookid=2567§ionid=207231878. 5. Kuo S-H. Ataxia. Continuum (Minneap Minn). 2019;25(4):1036-1054. 6. Bird TD. Hereditary ataxia overview. In: Adam MP, Ardinger HH, Pagon RA, et al, eds. GeneReviews® [Internet]. University of Washington, Seattle. Revised July 25, 2019. 7. Ashizawa T, Xia G. Ataxia. Continuum (Minneap Minn). 2016;22(4):1208-1226. 8. de Silva RN, Vallortigara J, Greenfield J, et al. Diagnosis and management of progressive ataxia in adults. Pract Neurol. 2019;19:196-207. 9. Perlman S. Hereditary ataxia overview. In: Adam MP, Feldman J, Mirzaa GM, et al, eds. GeneReviews® [Internet]. University of Washington, Seattle. Revised September 12, 2024. 10. Schulz JB, Boesch S, Bürk K, et al. Diagnosis and treatment of Friedreich ataxia: a European perspective. Nat Rev Neurol. 2009;5(4):222-234. 11. Fogel BL, Perlman S. Clinical features and molecular genetics of autosomal recessive cerebellar ataxias. Lancet Neurol. 2007;6(3):245-257. 12. Lynch DR, Farmer JM, Balcer LJ, Wilson RB. Friedreich ataxia: effects of genetic understanding on clinical evaluation and therapy. Arch Neurol. 2002;59(5):743-747. 13. Perlman SL. Evaluation and management of ataxic disorders: an overview for physicians. National Ataxia Foundation. 2016. 14. Deutsch EC, Santani AB, Perlman SL, et al. A rapid, noninvasive immunoassay for frataxin: utility in assessment of Friedreich ataxia. Mol Genet Metab. 2010;101(2-3):238-245. 15. Galea CA, Huq A, Lockhart PJ, et al. Compound heterozygous FXN mutations and clinical outcome in Friedreich ataxia. Ann Neurol. 2016;79(3):485-495. 16. Lynch DR, Schadt K, Kichula E, McCormack S, Lin KY. Friedreich ataxia: multidisciplinary clinical care. J Multidiscip Healthc. 2021;14:1645-1658. 17. Delatycki MB, Bidichandani SI. Friedreich ataxia—pathogenesis and implications for therapies. Neurobiol Dis. 2019:132:104606. 18. Sawcer S, Franklin RJM, Ban M. Multiple sclerosis genetics. Lancet Neurol. 2014;13(7):700-709. 19. Fox RJ, Cohen JA. Multiple sclerosis: the importance of early recognition and treatment. Cleve Clin J Med. 2001;68(2):157-171. 20. Mincu RI, Magda LS, Florescu M, et al. Cardiovascular dysfunction in multiple sclerosis. Maedica (Bucur). 2015;10(4):364-370. 21. Patsopoulos N. Genetics of multiple sclerosis: an overview and new direction. Cold Spring Harb Perspect Med. 2018;8(7):a028951. 22. Bird TD. Charcot-Marie-Tooth hereditary neuropathy overview. In: Adam MP, Feldman J, Mirzaa GM, et al, eds. GeneReviews® [Internet]. University of Washington, Seattle. Revised April 25, 2024. 23. Orphanet. Charcot-Marie-Tooth disease type 1. Revised January 20, 2025. Accessed January 31, 2025. https://www.orpha.net/en/disease/detail/65753. 24. Hwang S, Park C, Kim R, et al. Cerebellar white matter abnormalities in Charcot-Marie-Tooth disease: a combined diffusion tensor imaging analysis. J Clin Med. 2021;10:4945. 25. Isner JM, Hawley RJ, Weintraub AM, Engel WK. Cardiac findings in Charcot-Marie-Tooth disease. Arch Intern Med. 1979;139:1161-1165. 26. National Institute of Child Health and Human Development. National Institutes of Health. What are the early signs of cerebral palsy? Revised May 11, 2021. Accessed January 31, 2025. https://www.nichd.nih.gov/health/topics/cerebral-palsy/conditioninfo/signs. 27. McHale DP, Jackson AP, Campbell DA, et al. A gene for ataxic cerebral palsy maps to chromosome 9p12–q12. Eur J Hum Genet. 2000;8(4):267-272. 28. Smithers-Sheedy H, Badawi N, Blair E, et al. What constitutes cerebral palsy in the twenty-first century? Dev Med Child Neurol. 2013;56(4):323-328. 29. National Institute of Neurological Disorders and Stroke. National Institutes of Health. Cerebral Palsy. Revised July 19, 2024. Accessed January 31, 2025. https://www.ninds.nih.gov/health-information/disorders/cerebral-palsy. 30. Fukuhara T, Namba Y, Yamadori I. Peripheral sensory neuropathy observed in children with cerebral palsy: is chronic afferent excitation from muscle spindles a possible cause? Childs Nerv Syst. 2010;26:751-754. 31. Jin SC, Lewis SA, Bakhtiari S, et al. Mutations disrupting neuritogenesis genes confer risk for cerebral palsy. Nat Genet. 2020;52(10):1046-1056. 32. Wallace SE, Bird TD. Molecular genetic testing for hereditary ataxia: what every neurologist should know. Neurol Clin Pract. 2018;8(1):27-32.